Research
Evidence Alignment Engine for Biopharma Target Validation and Translational Research
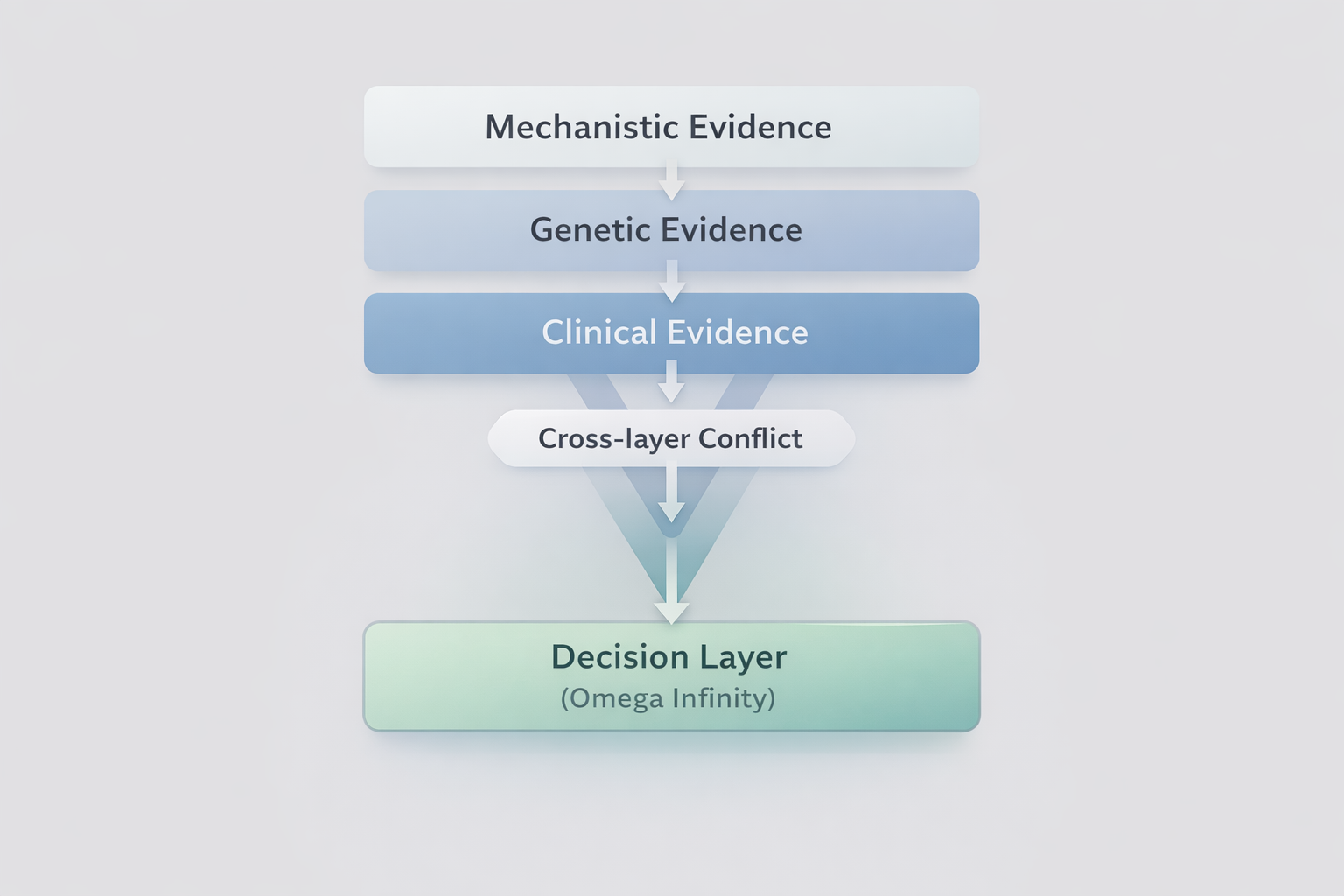
A structured evidence engine for biomedical research. Organize mechanistic, clinical, and genetic evidence into inspection-ready Evidence Alignment.
- Mechanistic, clinical, and genetic evidence
- Structured Evidence Alignment assembly
- Explicit uncertainty and limitation framing
- T / Φ / Σ diagnostics